We were tasked to post questions about enterprise architecture and others as it relates to health. Below are my questions, and answers from Dr. Alvin Marcelo, and a few others.

#1 Is interoperability addressed by using open EHR?
See Doctors Find Barriers to Sharing Digital Medical Records http://www.nytimes.com/2014/10/01/business/digital-medical-records-become-common-but
Marcelo: In the US, the EMRS got bigger before the Health Information Exchanges (the interoperability layer). In such a situation, it becomes harder for mature EMRS to connect “back” to an HIE. The lesson is to quickly define the HIE and ask the EMRs to comply with it.
Up to a certain point [interoperability can be addressed by open EHRs] but not beyond it. OpenEHR helps organize clinical knowledge and structure it consistently. That helps with managing the complexity of clinicians having varying ways of representing their knowledge … [In an openEHR workshop, group] members given the same clinical scenario …had varying mindmaps for that case. If they proceeded to create the EMRs from their mindmap, for sure, their EMRs will not be interoperable because they had already diverged at the clinical knowledge layer (in EA, the business architecture). OpenEHR is like a bucket of lego blocks from where you can get pre-built blocks (representing clinical knowledge) which you can then put together to create your EMR. Since all of you got your building blocks from the same bucket, the chances that your EMRs can connect to each other is higher.
#2 Will open EMR prevent this type of scenario?
See Billing Dispute Leads to Blocked Patient Data in Maine. http://www.bostonglobe.com/news/nation/2014/09/21/electronic-health-records-vendor-compugroup-blocks-maine-practice-from-accessing-patient-data/6ILpMv78NARDsrdU5O0T9N/story.html?event=event25
Marcelo: No it will not. There are at least three layers of interoperability that need to exist before data flows effectively — business, information, technical. Open electronic medical records can address information and technical interoperability but cannot assure that there will be business interoperability (that is, two entities agreeing to do business with each other). The article is interesting that it actually states that information and technical interoperability already existed but a disagreement in how to run the business prevented the exchange of information. Similar cases abound in healthcare.
ITITan: I saw one contract where it is explicitly stated that there is an extra charge for extracting records at end of contract.
PSantiago: Is this practice fusion?
ITITan: It was a local EMR product
AJReyes: Have installed openemr and giving it a good look. What do you think about it?
PSantiago: I am suspicious of a hidden agenda… Whats in it for them? I don’t know yet, still exploring…
AJReyes: FOSS is like that. They may make money from professional support, or from having it in their CV or they just enjoy doing it. Still the data model is open to you (mysql RDBMS) so in theory, you should not get stuck, the way Full Circle was. FOSS aside, Full Circle should know, doctor lang ang puwedeng pilitin mag T.Y.
MAAlcantara-Santiago If you are implementing the openEMR in your own institution or hospital by “yourself” (meaning there is no third party implementor), then no, it should not be a problem.
But, in cases where you have a third party implementor of openEHR, then the problem of this happening in your institution will depend on the contract. In this case, it doesn’t matter if its openEMR or not. What matters is what is stated in the contract. If the institution failed to correct an implementor’s stated penalty wheb the institution is not able to pay, then the legal department of that institution is incompetent. I would rather not do business with an implementor that holds access to information when problems with payment or financials are experienced.
Sorry have to correct myself on this. I meant openMRS and not openEHR. OpenEMR is the open source EMR. OpenHR is a standards tool and contains concepts or archetypes which can be used in any EMR.
But, the problem of information lockdown is still dependent on the contract between implementor and the institution.
AHSantiago This is not an issue of implementing another system or not just to solve the problem. This is just a simple question of is this stipulated in the contract between vendor and client. In the world of entrepreneurship, if a businessman owns a bank money that he used for his business and does not pay back the bank can take back what is rightfully theirs in any form in which will be stated in their contract. This is like what happened between stradcom and lto, where system access was used as a bargaining chip to complete the payment deal. I think LTO won legally
AJReyes If you choose to run the system on your own computers, as opposed to having someone else host them, you should always be able to use it, even as a second system (inconvenient). Given the quality of our broadband system, I doubt if any local would seriously consider outside hosting. As to importing the data to a new system so you can have seamless access, the base implementation of openemr has over 170 tables but only for form* tables, and a few others have the clinical data so it’s doable by an independent provider but only if your contract is big enough. Would it retain it’s legal validity? The advantage of FOSS is that you can fire your support staff and hire another group if need be.
PPlanas This is what the IT department is for you back-up your data, so that whatever the local EMR vendor wants between you and management, regardless of the legalities, continuity of care can still be done on another EHR. Just implement a business continuity plan for vendor related lock-ups.

#3 Should PGH adopt an IT governance and an enterprise architecture? Or are we in the middle of it? What are our barriers?PGH has a wealth of clinical data but is not a DOH hospital. How can we harvest this data or integrate with the DOH system?
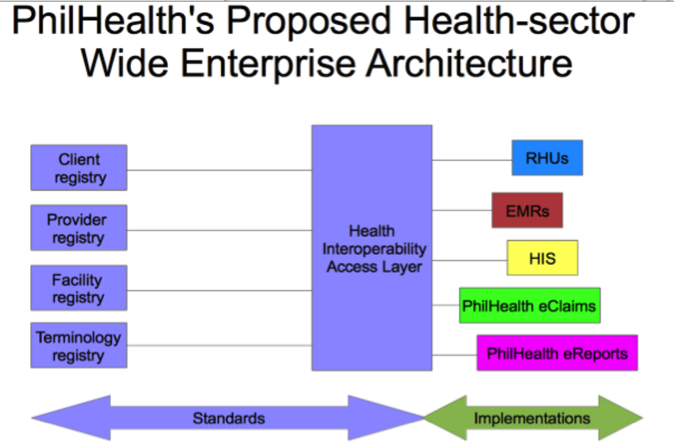
THerbosa: Through an interoperability layer. Mela Lapitan onboard
TLeachon: Just met with Atty Deegee, Staff of Sen Pia, She asked how to support this.
#4 Can we make all departments’ EHR/EMR interoperate so we get a better picture of our patients in PGH? First things first, EHRs for different departments in PGH, make them interoperable and fully accessible by health care provider?
Marcelo: First definitions: an EMR is an electronic system for recording patient data in one facility. An EHR on the other hand is a person’s longitudinal record which may comprise of data coming from different EMRs. So in PGH, ISIS is the EMR of the Department of Surgery. In IM, they have their own EMR. But patient Juan dela Cruz should only have one EHR which is a collection of his data from Surgery and IM.
How is this possible? Through interoperability — a system that allows the collection of Juan’s data from the different EMRs where his data resides. Do we need to design this from scratch? No, the Integrating the Healthcare Enterprise (www.ihe.net) has already described how this could be done in a health system.

#5 Practice Fusion claims free electronic health records, “no hidden costs, no strings attached.” Really? Is there a hidden agenda? Practice fusion sells “anonymised data.” Are we as physicians willing to take that risk?
From Practice Fusion Privacy Policy: http://www.practicefusion.com/pages/privacy-policy.html
“We use non-personal information for the following purposes: Auditing, research, measurement and analysis in order to maintain, administer, enhance and protect our Services, including analyzing usage trends and patterns and measuring the effectiveness of content, advertising, features or services; Creating new features and services; Contextual and cookie-based automated content delivery, such as tailored ads or search results;Health and medical research; public health and service activities; healthcare- and medical-related services; and Other purposes described in this Policy or your User Agreement.
We may also use non-personal information to prepare aggregate reports for current or future advertisers, sponsors or other partners to show trends about the general use of our Services. Such reports may include age, gender, geographic, demographic or other general user information, but do not include personal information.”
Marcelo: Everyone has a hidden agenda, (deliberately or not). The key is agreeing on principles. Based on Data Privacy Act of 2012, personal information is not sharable….except when anonymized for research… so technically, practice fusion is above the table… (I have no stocks with PF).
#5a If data is anonymised for market research, and not health research, such as pharmaceuticals establishing trends and analysing physicians’ practice patterns, is this still acceptable?
Marcelo: Based on the Data Privacy Act of 2012 (Chapter 1, Section 4 (d)), processing personal information for “research purposes” is allowed by law. As the section states, “research purpose” is out of scope of the Act. But is it acceptable (who defines “acceptable)? (Make sure to consult a lawyer prior to implementing this for your protection).
“SEC. 4. Scope. – This Act applies to the processing of all types of personal information and to any natural and juridical person involved in personal information processing including those personal information controllers and processors who, although not found or established in the Philippines, use equipment that are located in the Philippines, or those who maintain an office, branch or agency in the Philippines subject to the immediately succeeding paragraph: Provided, That the requirements of Section 5 are complied with.
This Act does not apply to the following:
(a) Information about any individual who is or was an officer or employee of a government institution that relates to the position or functions of the individual, including:
(1) The fact that the individual is or was an officer or employee of the government institution;
(2) The title, business address and office telephone number of the individual;
(3) The classification, salary range and responsibilities of the position held by the individual; and
(4) The name of the individual on a document prepared by the individual in the course of employment with the government;
(b) Information about an individual who is or was performing service under contract for a government institution that relates to the services performed, including the terms of the contract, and the name of the individual given in the course of the performance of those services;
(c) Information relating to any discretionary benefit of a financial nature such as the granting of a license or permit given by the government to an individual, including the name of the individual and the exact nature of the benefit;
(d) Personal information processed for journalistic, artistic, literary or research purposes;
(e) Information necessary in order to carry out the functions of public authority which includes the processing of personal data for the performance by the independent, central monetary authority and law enforcement and regulatory agencies of their constitutionally and statutorily mandated functions. Nothing in this Act shall be construed as to have amended or repealed Republic Act No. 1405, otherwise known as the Secrecy of Bank Deposits Act; Republic Act No. 6426, otherwise known as the Foreign Currency Deposit Act; and Republic Act No. 9510, otherwise known as the Credit Information System Act (CISA);
(f) Information necessary for banks and other financial institutions under the jurisdiction of the independent, central monetary authority or Bangko Sentral ng Pilipinas to comply with Republic Act No. 9510, and Republic Act No. 9160, as amended, otherwise known as the Anti-Money Laundering Act and other applicable laws; and
(g) Personal information originally collected from residents of foreign jurisdictions in accordance with the laws of those foreign jurisdictions, including any applicable data privacy laws, which is being processed in the Philippines.”